Citation Information
Han and Kang, J Life Sci, Vol. 3, No. 2, February 2026:1-5 [https://doi.org/qqkj]
Bone marrow is both a primary site of blood cell production and a frequent site of cancer spread, particularly in breast cancer. Anemia, a conditioned characterized by red blood cell (RBC) deficiency, is common in patients with bone metastases, in which cancer cells spread from the original tumors to the bones, but the underlying mechanisms of how they are connected are not well defined. Using an in vivo proximity-labelling system in a living organism, combined with single-cell RNA sequencing, a method that takes a ‘snapshot’ of what each individual cell is doing by measuring its gene activity based RNA express levels, we identified a rare population of macrophages (immune cells that act as "clean-up crew") with iron recycling features that are enriched in the breast cancer bone metastatic niche. Under normal conditions, these macrophages support erythropoiesis, the process of making RBCs, by recycling iron for RBC production. In the metastatic setting, however, tumor cells hijack these macrophages to obtain iron, impairing their ability to sustain RBC formation and contributing to anemia. In response to limited oxygen and iron availability, metastatic tumor cells display striking plasticity, an ability to change its cellular identity and behavior in response to its environment, by acting like erythroblasts, the RBC precursors. This “erythroblast mimicry” helps tumor cells adapt to the hypoxic (low-oxygen) bone marrow microenvironment.
Importantly, iron-handling macrophages with similar transcriptional features to those identified in our mouse models were also found in human bone metastases, and elevated hemoglobin (Hgb) expression in tumor cells was associated with increased risk of bone metastasis. Our findings reveal a previously unrecognized role of iron-recycling macrophages in the bone metastatic niche and uncover a previously unrecognized tumor–immune–metabolic axis that accelerates bone metastasis progression and contributes to cancer-associated anemia.
Keywords : Bone metastasis, macrophage, breast cancer, anemia, iron metabolism, hypoxia.
Background :
More than 150,000 people in the U.S. are living with metastatic breast cancer1. Around 70% of them develop bone metastases, which can cause severe pain, bone fractures, and other serious complications that affect both survival and quality of life2. Development of bone metastasis relied on the so-called “seed and soil” interactions, a hypothesis proposed by British Surgeon Dr. Stephen Padget which suggests that cancer cells (the “seeds”) thrive in supportive environments (the “soil”)3. Most previous work on bone metastasis has focused on the cancer cells themselves—what makes these seeds so good at growing in bone4,5. Much less is known about the “soil”: the specialized cells and signals in the bone marrow that help or hinder tumor growth.
Anemia, when the body has too few red blood cells to carry oxygen, can leave patients feeling persistently tired, weak, and short of breath6. It is common in people with breast cancer that has spread to the bone7. However, earlier explanations were largely “macroscopic”: as tumor cells grow in the bone marrow, they physically crowd out normal blood-forming cells, reducing red blood cell (RBC) production and leading to anemia8. Understanding how bone metastases drive anemia could enable more targeted ways to treat it, improving both quality of life and survival of cancer patients.
Our Main Findings :
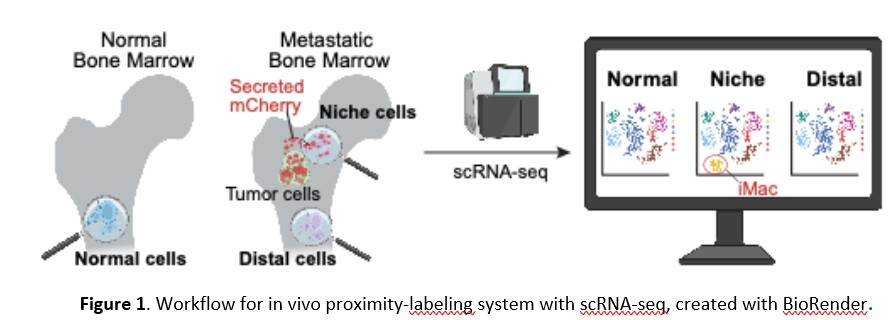
In this study9, we used advanced single-cell RNA sequencing (scRNA-seq) together with an in vivo proximity-labeling system10 that marks cells located close to tumor cells. Briefly, tumor cells were engineered to secrete mCherry, a fluorescent protein, and delivered to the mouse bone marrow. In the metastatic mouse, bone marrow cells located near tumor cells (“niche cells”) become mCherry-labeled, whereas cells farther away (“distal cells”) remain unlabeled. Bone marrow cells from healthy mouse were included as normal controls (“normal cells”) for scRNA-seq. This allowed us to systematically map the bone metastatic microenvironment (the “soil”) and identify which types of cells cluster around metastatic tumors in the bone marrow.
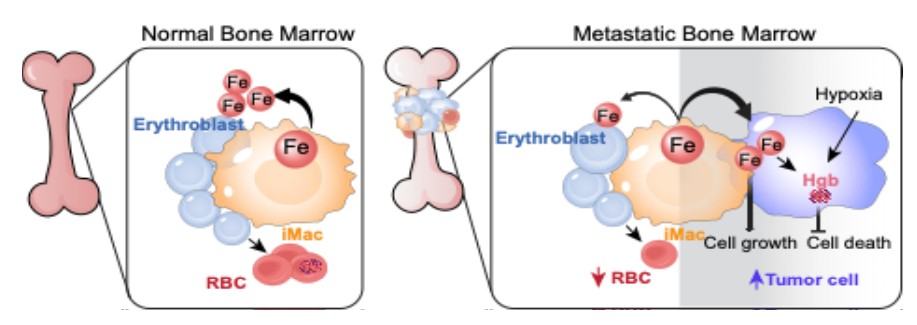
We discovered a rare population of iron-recycling macrophages (iMac) that normally surrounded by RBC precursors and help recycle iron from old RBCs so new ones can be made11. In the setting of bone metastasis, these macrophages become highly enriched in the vicinity of tumor cells. Because cancer cells require large amounts of iron to grow and divide, our data suggest that tumor cells hijack iMac to gain access to iron. This “iron theft” disrupts normal RBC production and contributes to anemia, a common but often poorly explained complication in patients with bone metastases.
We also found that tumor cells adapt even further to the harsh bone marrow environment. In response to low oxygen, they begin to mimic erythroblasts, the RBC precursors, by turning on hemoglobin production. This unusual “erythroblast-like” program appears to help tumor cells survive and thrive in an environment that would otherwise be difficult for them.
Story Behind the Discovery
This study was driven by both clinical urgency and unexpected personal experiences. Using cutting-edge in vivo niche labelling and single-cell RNA sequencing, we sought to understand how the bone marrow microenvironment facilitates cancer metastasis. Along the way, we uncovered a striking and clinically underappreciated connection: patients with bone metastases frequently suffer from anemia, yet it is often left untreated12. This gap in care prompted us to explore how the tumor microenvironment contributes to anemia—not simply as a byproduct of disease, but as a process intimately tied to the biology of metastasis.
The initial insight linking these macrophages to anemia arose from a seemingly unrelated personal moment. At the time we first analyzed our RNA-seq data characterizing niche-specific macrophages, Yujiao had just received routine blood test results showing mild iron-deficiency anemia, which was corrected with dietary changes and iron supplements. At the same time Yujiao noticed that this macrophage cluster showed a strong transcriptional signature related to heme metabolism—the very term Yujiao had been reading about while trying to understand her own lab results. The parallel between her clinical bloodwork and the mouse phenotypes became a “eureka moment,” suggesting that these macrophages might connect metastasis to anemia through heme and iron metabolism.
At the same time, Yibin was training for an Ironman triathlon race and paying close attention to his own iron levels, a concern common among endurance athletes due to chronic losses through sweat, hemolysis, and gastrointestinal microbleeds. This made iron metabolism a recurring topic in our casual lab discussions and underscored how delicate the balance of iron availability is, both in athletic performance and disease. In a stroke of scientific humor, we realized that the macrophage population we were studying, labelled IronMac or “iMac” for iron macrophage in the manuscript, coincided amusingly with the IronMan shirts that now dominate Yibin’s wardrobe.
The convergence of these scientific insights and personal experiences gave us a unique lens to understand the interplay between metastasis and anemia. Tumor cells in the bone marrow niche were not only exploiting iMac for iron, but were also adapting to the hypoxic environment by upregulating erythroblast-like features, including hemoglobin production, suggesting a striking form of phenotypic mimicry.
Together, these observations led us to uncover a previously unrecognized mechanism linking immune modulation, iron metabolism, and tumor plasticity in metastatic progression and anemia. They also raised an important therapeutic question: could targeting niche macrophages or the iron-transfer pathway limit metastasis while simultaneously alleviating anemia?
Conclusion :
Our study shows that when breast cancer cells spread to the bone, they can steal iron from specialized iron-recycling macrophages that normally support RBC production. This iron theft helps tumors grow but undermines the bone marrow’s ability to make new RBCs, contributing to anemia. Meanwhile, tumor cells adapt by adopting features of RBC precursors and synthesizing hemoglobin, allowing them to endure hypoxia.
These findings improve our understanding of how metastatic tumor cells exploit the bone marrow “soil,” reveal how they can change their identity to survive, and suggest a new mechanism behind bone metastasis–associated anemia. These insights may ultimately guide the development of new therapies that protect bone marrow function and reduce complications such as anemia, while limiting tumor growth in bone. The involvement of this iron transfer characteristic was validated in human bone metastasis samples from multiple cancer types, highlighting its broad translational relevance. This discovery not only enhances our understanding of tumor plasticity and metabolic adaptation in the bone metastatic niche but also identifies potential mechanism underlying cancer-associated anemia. Targeting this metabolic crosstalk could enable new therapies that curb tumor growth while preserving bone marrow function and easing anemia, a frequently overlooked yet debilitating complication of metastatic breast cancer. Such approaches hold promise for improving both survival and quality of life for patients by addressing tumor progression and offering more effective and safer supportive care.
Statement :
YH and YK co-wrote and approved the manuscript.
YH was supported by the Charles H. Revson Senior Fellowship in Biomedical Science and YK was supported by grants from the American Cancer Society (RP-19-180-01-CSM), Ludwig Cancer Research, Brewster Foundation, Breast Cancer Research Foundation and Susan G. Komen Foundation.
YH declares no competing interests. YK is a co-founder and chair of Scientific Advisory Board of Firebrand Therapeutics, Inc and Kayothera, Inc.
References :
1. Mariotto, A.B., Etzioni, R., Hurlbert, M., Penberthy, L., and Mayer, M. (2017). Estimation of the Number of Women Living with Metastatic Breast Cancer in the United States. Cancer Epidemiol Biomarkers Prev 26, 809-815. 10.1158/1055-9965.Epi-16-0889.
2. Mayer, D.K., Struthers, C., and Fisher, G. (1997). Bone metastases: Part II--Nursing management. Clin J Oncol Nurs 1, 37-44.
3. Paget, S. (1989). The distribution of secondary growths in cancer of the breast. 1889. Cancer Metastasis Rev 8, 98-101.
4. Jehanno, C., Vulin, M., Richina, V., Richina, F., and Bentires-Alj, M. (2022). Phenotypic plasticity during metastatic colonization. Trends Cell Biol 32, 854-867. 10.1016/j.tcb.2022.03.007.
5. Han, Y., and Kang, Y. (2022). Bone niche and bone metastases. In Bone Sarcomas and Bone Metastases-From Bench to Bedside, (Elsevier), pp. 107-119.
6. Birgegård, G., Aapro, M.S., Bokemeyer, C., Dicato, M., Drings, P., Hornedo, J., Krzakowski, M., Ludwig, H., Pecorelli, S., Schmoll, H.-J., et al. (2005). Cancer-Related Anemia: Pathogenesis, Prevalence and Treatment. Oncology 68, 3-11. 10.1159/000083128.
7. Demir, L., Akyol, M., Bener, S., Payzin, K.B., Erten, C., Somali, I., Can, A., Dirican, A., Bayoglu, V., Kucukzeybek, Y., et al. (2014). Prognostic Evaluation of Breast Cancer Patients with Evident Bone Marrow Metastasis. The Breast Journal 20, 279-287. https://doi.org/10.1111/tbj.12264.
8. Makoni, S.N., and Laber, D.A. (2004). Clinical spectrum of myelophthisis in cancer patients. American journal of hematology 76, 92-93.
9. Han, Y., Sarkar, H., Xu, Z., Lopez-Darwin, S., Wei, Y., Hang, X., Liu, F., Tran, K., Wang, W., Miller, J.M., et al. (2025). Tumors hijack macrophages for iron supply to promote bone metastasis and anemia. Cell 188, 6335-6354 e6326. 10.1016/j.cell.2025.08.013.
10. Ombrato, L., Nolan, E., Kurelac, I., Mavousian, A., Bridgeman, V.L., Heinze, I., Chakravarty, P., Horswell, S., Gonzalez-Gualda, E., Matacchione, G., et al. (2019). Metastatic-niche labelling reveals parenchymal cells with stem features. Nature 572, 603-608. 10.1038/s41586-019-1487-6.
11. Li, W., Guo, R., Song, Y., and Jiang, Z. (2020). Erythroblastic Island Macrophages Shape Normal Erythropoiesis and Drive Associated Disorders in Erythroid Hematopoietic Diseases. Front Cell Dev Biol 8, 613885. 10.3389/fcell.2020.613885.
12. Gilreath, J.A., and Rodgers, G.M. (2020). How I treat cancer-associated anemia. Blood 136, 801-813. 10.1182/blood.2019004017.
Authors :
Dr. Yibin Kang is a Warner-Lambert/Parke-Davis Professor of Molecular Biology at Princeton University, New Jersey, USA.

Yujiao Han Dr Yujiao Han is a postdoctral fellow at the Department of Molecular Biology, Princeton University, New Jersey
Reviewers :

Dr. Austin Arrigo Postdoctoral Associate at the University of Pittsburgh, at Magee Women's Research Institute studying high grade serous ovarian cancer. Dr. Arrigo is a postdoc reviewer at JoLS-Pub

Ms. Ghaffarian Zavarzadeh Parisima is a PhD student at the East Tennessee State University. Her expertise lies in Cancer, Neurodegenerative disorders, Biomarker development, Drug repurposing and Bioinfomratics. She is a grad student reviewer at JoLS-Pub.

Ms. Neha Ramasastry graudated from the University of California at Riverside, majoring in neuroscience. Neha is an Editorial Coordinator at JoLS-Pub. She coordinated the review process of this summary.